Smoke and rumor often rise together in Lebanon. This week, both did-from an unexpected place-after a blaze reportedly broke out near an underground site said to be linked to Hezbollah’s finances. The incident has stirred a swirl of claims and counterclaims: that a concealed bunker beneath a hospital held a cache of gold and cash worth hundreds of millions of dollars, that the fire exposed more than it destroyed, and that the truth lies somewhere between secrecy and spectacle.
Hezbollah has not confirmed the allegations, independent verification remains scarce, and official statements so far are cautious. Yet the story’s contours touch fault lines that are all too familiar: the movement’s opaque funding streams amid international sanctions, the use and abuse of civilian spaces in a country frayed by crisis, and the enduring figure of Hassan Nasrallah-whose name, in friend and foe alike, evokes both steadfastness and shadow.
Whether the blaze was accident or act, and whether the sums cited are real or inflated, the episode forces a set of uncomfortable questions into the open. What lies beneath the surface of Lebanon’s public life-its hospitals, its neighborhoods, its politics-when militancy, governance, and survival are layered so closely together? As investigators pick through ash and allegation, the fire’s heat may prove less consequential than the light it casts.
From smoke to ledger inside the reported fire at an alleged Hezbollah gold site
Witnesses describe a blaze licking through a nondescript industrial block, its heat bending rebar and turning vault paint to ash. What the fire may have exposed, however, reaches beyond scorched metal: a web of inventories, intermediaries, and quiet ledgers that allegedly tied the site to clandestine bullion flows. Local outlets circulated images of warped safes and charred notebooks; others claimed melted doré bars and assay slips were recovered-none independently verified. Officials offered sparse detail as crews dampened hot spots, while rival media amplified competing narratives about ownership, purpose, and the money trail said to run beneath the smoke.
| Claim | Status | Notes |
|---|---|---|
| Gold-processing activity on-site | Contested | Footage and reports unverified |
| Large cash/bullion cache under a medical facility | Alleged | No public proof; official inquiry requested |
| Cause of the fire | Unknown | Investigators have not concluded |
| Documented financial ledgers recovered | Unclear | Conflicting media accounts |
Forensic accounting in such cases follows the heat signature of finance more than flame: assay certificates, refinery intake logs, shipping manifests, and energy-consumption anomalies can sketch a ledger of intent. If authorities proceed, they’ll likely cross-reference customs entries, vault access records, and insurer declarations against telecom pings and warehouse utilities to test the narrative. In the meantime, the public record remains provisional, and separating smoke from signal will hinge on verifiable documents and chain-of-custody disclosures.
- What’s known: A fire occurred; official conclusions are pending.
- What’s alleged: Gold-linked operations and a significant hidden cache.
- What to watch: Satellite thermal data, insurer filings, refinery statements.
- Key voices: Local authorities, hospital administrators, independent auditors.
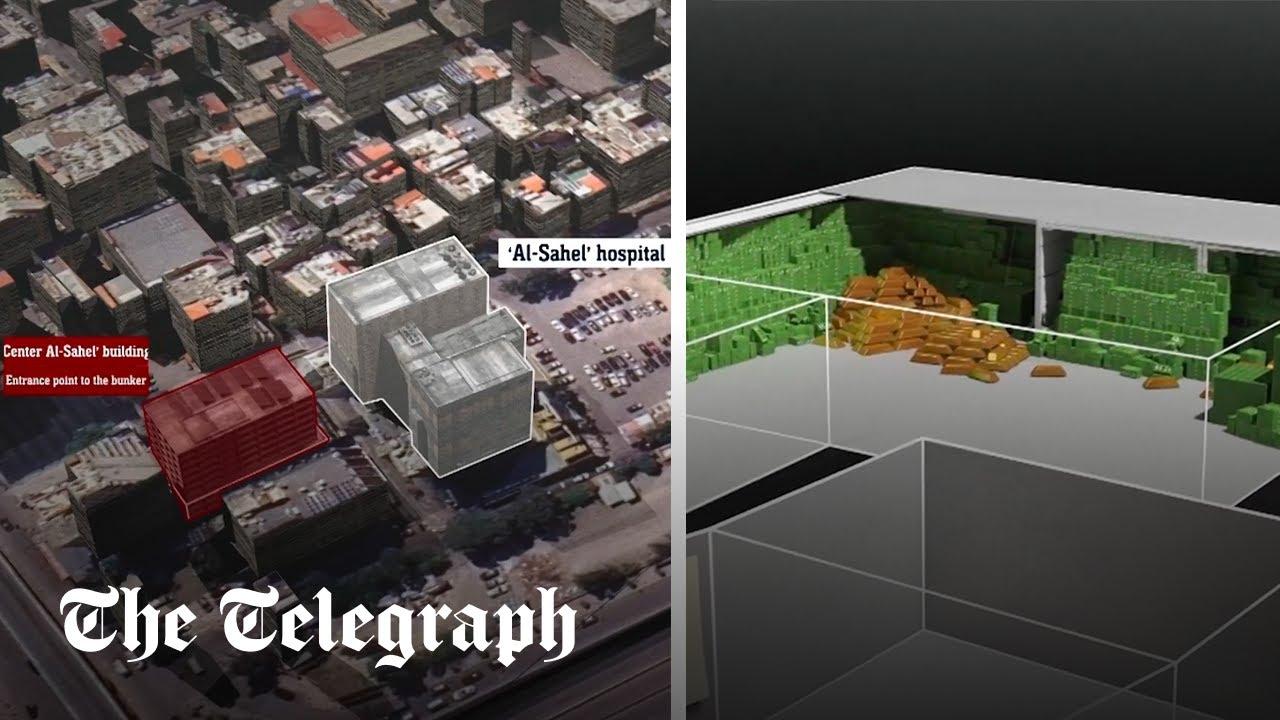
Probing claims of a bunker beneath a hospital and a half billion in assets
The blaze set off a storm of allegations, centering on a fortified chamber said to sit beneath a busy medical complex and to have safeguarded vast stores of cash, bullion, and sensitive media. Officials and hospital administrators deny the narrative; advocates warn of rumor-driven harm. Yet local engineers point to unusual power loads and reinforced sublevels typical of civil-defense shelters, while residents recall nocturnal deliveries and sealed service shafts. The picture is fragmentary: a collage of documents of uncertain provenance, satellite tiles with ambiguous shadows, and whispers of off-ledger wealth-intriguing, but not dispositive.
- What to verify: original floor plans, utility schematics, maintenance logs, and contractor permits.
- Site forensics: heat-mapping of the burn, residue analysis, fault lines in concrete, and elevator shaft integrity.
- Financial trail: audited ledgers, donor flows, cross-border transfers, bullion receipts, and beneficial ownership records.
- Safeguards: patient safety corridors, medical neutrality, chain-of-custody for evidence, and independent observers.
| Claim | Evidence snapshot | Confidence | Notes |
|---|---|---|---|
| Sublevel facility exists | Civil defense blueprint (2014) | Medium | May be a shelter |
| Assets ≈ $500M stored | Anonymous ledger images | Low | Requires audit |
| Dedicated power/fiber | Utility load spikes | Medium | Alt uses plausible |
| Security retrofits | Reinforced door invoices | Medium | Not uncommon |
| Fire origin: service tunnel | Prelim incident memo | Low | Await lab tests |
The stakes are acute: hospitals must remain protected spaces, and investigations must not compromise care or civilian safety. Any publication should foreground corroboration over virality, weigh alternative explanations, and separate emergency infrastructure from covert use with on-record proof. A disciplined approach-transparent sourcing, independence from parties to the conflict, and verifiable timelines-helps filter heat from light, ensuring that if an underground cache or command space truly existed, it is demonstrated by evidence rather than amplified by speculation.

Humanitarian and legal stakes medical neutrality and civilian protection
Reports that a fortified cash depot and command space may have been embedded beneath a medical facility pose urgent questions about medical neutrality and the duty to shield civilians from harm. Under the Geneva Conventions and customary international humanitarian law, hospitals and clinics remain protected spaces; even when misused, protection is lost only if they are employed for acts harmful to the enemy, and only after a clear warning and a reasonable time limit go unheeded, with any response still bound by necessity, distinction, and proportionality. Conversely, militarizing a hospital and endangering patients, staff, and the surrounding population can itself constitute a violation. In such contested narratives, the law requires independent verification, meticulous documentation, and accountability mechanisms that prioritize life over tactical advantage.
- Do not attack medical units, transports, or marked facilities; respect deconfliction arrangements.
- Do not militarize healthcare sites or use patients and staff as shields.
- Issue effective warnings and allow time for evacuation if hostile use is credibly established.
- Facilitate access for emergency services, ICRC/neutral monitors, and safe corridors for patients.
- Record decisions: target validation, warnings, evacuation attempts, and proportionality assessments.
- Preserve evidence and enable impartial investigations into all alleged violations.
| Issue | Lawful Focus | Red Lines |
|---|---|---|
| Hospital protection | Distinction, warnings, proportionality | Direct attacks on medical units |
| Alleged hostile use | Verified evidence, time-bound warning | Assumptive strikes, collective punishment |
| Civilian evacuation | Safe corridors, medical triage | Blocking ambulances/fire crews |
| Financial assets on-site | Judicial seizure, chain of custody | Pillage, reprisal theft |
The humanitarian north star is constant: protect civilians first. Fires near life-sustaining infrastructure magnify risk, from oxygen explosions to mass displacement and care interruptions. Practical safeguards-ceasefire windows for responders, redundant power/oxygen supplies, patient tracking, and trauma-informed evacuation-can save lives regardless of who is accused of what. Whether allegations of covert treasure hoards or command bunkers prove true or not, the lawful path is the same: keep care spaces sacrosanct, investigate impartially, and center every operational decision on minimizing foreseeable civilian harm.
Recommendations for independent verification asset tracing and safeguarding healthcare facilities
Independent verification in conflict-affected contexts must balance evidentiary rigor with the primacy of patient safety. Establish a documented chain of custody from the first observation to final archiving; apply triangulation (on-the-ground testimony, OSINT, and remote sensing) to reduce single-source bias; and ensure medical neutrality by placing clinical leadership at the center of access decisions. Use structured geolocation and chronolocation for media, verify metadata, and corroborate with multiple sensor modalities (imagery, thermal, acoustic) where feasible. All collection should follow data minimization and privacy-by-design, redacting patient identifiers and sensitive clinical layouts while preserving probative value for auditors and courts.
- Neutral lead: Appoint a cross-recognized, nonpartisan coordinator (medical NGO + technical lab).
- Evidence controls: Time-stamped inventories, tamper-evident seals, dual-key custody for rooms and lockers.
- Multisource checks: Satellite tasking, open-source imagery, and staff interviews mapped to one timeline.
- Clinical oversight: A hospital ethics board approves routes, timing, and blackout zones to avoid disrupting care.
- Transparent reporting: Publish a redacted verification brief with methods, limitations, and confidence levels.
| Role | Action | Output |
|---|---|---|
| OSINT Lab | Geo/chronolocate media | Imagery pack |
| Forensic Accountant | Trace flows, counterparties | Trail map |
| Hospital Compliance | Protect patients, privacy | Safety plan |
| IHL Advisor | Deconfliction & no-strike | Legal memo |
Asset tracing should combine financial intelligence with lawful, proportionate field procedures, keeping caregiving spaces protected. Apply AML/CFT frameworks, sanctions screening, and beneficial ownership mapping; cross-check bullion serials, assay certificates, customs codes, and warehouse receipts; and, where relevant, deploy blockchain analytics to follow tokenized or proxy value. Parallel to that, harden hospitals through deconfliction hotlines, live-updated No-Strike Lists, and continuity-of-care measures (redundant power, sterile corridors, blast-resistant glazing). Establish whistleblower channels, document retention schedules, and rapid, reversible scene controls that never impede urgent treatment.
- Data-sharing MOUs between auditors, regulators, and medical NGOs with strict access tiers.
- On-site controls: Zoned access, body-worn cameras for verifiers, and privacy masking for wards.
- Supply-chain probes: Refineries, logistics hubs, couriers-short, documented interviews and spot checks.
- Protective posture: Wayfinding for safe corridors, triage buffers, and patient evacuation drills.
- Accountability loop: Time-bound findings, right of reply, and an appeals channel for contested facts.
In Summary
As the smoke thins, the questions grow thicker. What exactly burned, who knew it was there, and why would any alleged cache-let alone a reported half-billion-dollar trove-sit beneath a place of care? Claims now collide with counterclaims, and verification lags behind the velocity of rumor.
What is clear is less the inventory than the implications. The incident sits at the tense intersection of clandestine finance, the laws of war, and the everyday precarity of civilians who live above the secrets others bury. It exposes the cost of opacity: when infrastructure of healing overlaps with infrastructure of conflict, everyone becomes more vulnerable.
In the coming days, independent inquiries and credible documentation-not whispers-will matter most. Until then, caution is a duty, not a hedge. When the embers finally cool, the real measure will not be the value of anything melted, but how much truth is recovered, how much accountability follows, and how firmly the line is redrawn between the places people trust and the shadows they fear.